For Healthcare Professionals:
Vestibular migraine (VM) and Ménière’s disease (MD) are common causes of recurrent vertigo attacks—and are clinically difficult to distinguish. This LMU study shows which features separate them best and where current diagnostic criteria (ICVD) reach their limits.
🔗Huppert D, Grill E, Becker-Bense S, Zwergal A, Strobl R. Diagnostic challenges in vestibular migraine-clinical differentiation from Menière’s disease and discrepancies with current classification criteria. J Neurol. 2025 Aug 5;272(9):558.
Study design:
- Site: LMU Munich (German Center for Vertigo and Balance Disorders, DSGZ)
- Participants: 276 patients (188 VM, 88 MD)
- Methods: history, audiometry, caloric testing, video head impulse test (vHIT), oculomotor tests
- Aim: identify clinical and instrumental features to differentiate VM and MD
Key results
- VM: more common in women (72%), earlier onset (mean ~40 years)
- MD: more common in men (49%), later onset (mean ~50 years)
- Ménière: typical spinning vertigo, tinnitus, hearing problems, nausea
- Vestibular migraine: more frequent headaches, light sensitivity, swaying/rocking dizziness
- Objective tests: MD more often showed caloric asymmetries and lower vHIT gain values
- Caloric–vHIT dissociation (abnormal calorics, normal vHIT) suggests MD
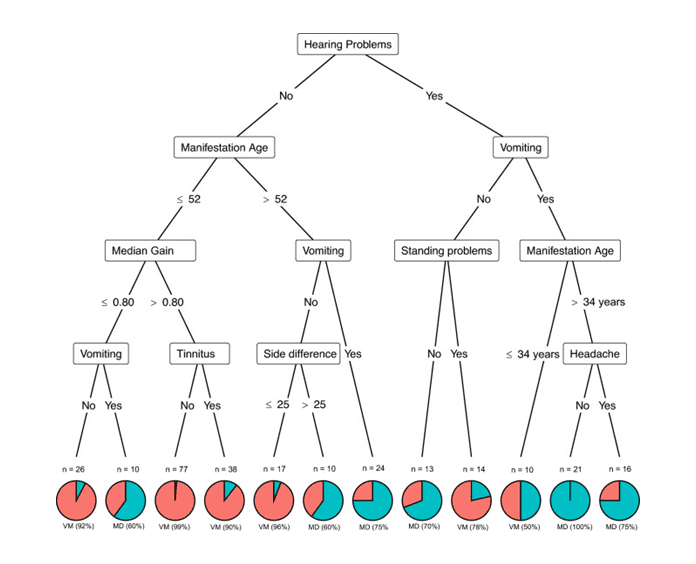
- Seven key criteria (86% accuracy): hearing problems, age, vomiting, caloric side difference, postural instability, tinnitus, headache (see figure below)
“Suspected VM” – when criteria don’t fit
About one third of VM cases did not fully meet ICVD criteria but were classified as VM by experts. Main reasons were atypical headache patterns (e.g., bilateral or pressure-like pain), a low number of attacks, differing accompanying symptoms, or subtle central oculomotor findings.
Clinical Relevance
- Not every patient matches the textbook picture—rigid criteria can easily lead to misdiagnosis.
- The best differentiation comes from combining history, caloric testing, vHIT, and clinical observation.
- “Suspected VM” should be taken seriously to avoid treatment delays.
Conclusion for Practice
Vestibular migraine and Ménière’s disease can be reliably distinguished using a small set of clinical and instrumental features. Structured history-taking, combined testing, and an open mind for atypical courses are essential.
👉 Are you interested in a comprehensive further training in vestibular rehabilitation and how you can provide therapeutic care and treatment for both conditions to help patients with dizziness faster and more safely?
Current further education opportunities can be found in the IVRT Course search.
For Patients – Easy to Understand
Vestibular Migraine or Ménière’s? Why both can feel similar—and yet are different
Two common causes of recurring vertigo attacks are vestibular migraine and Ménière’s disease. They can feel similar—but they arise for different reasons and often need different treatments.
📄 Huppert D, Grill E, Becker-Bense S, Zwergal A, Strobl R. Diagnostic challenges in vestibular migraine-clinical differentiation from Menière’s disease and discrepancies with current classification criteria. J Neurol. 2025 Aug 5;272(9):558. doi: 10.1007/s00415-025-13291-x. PMID: 40762827; PMCID: PMC12325411.
What does the new study show?
- Ménière’s: more often spinning vertigo, tinnitus, and hearing loss
- Vestibular migraine: often headache, light sensitivity, or a pressure-like feeling in the head
- With special tests (calorics, vHIT), doctors correctly distinguished the two in 86% of cases
Some people don’t fit neatly into textbook definitions. When typical migraine signs are missing or attacks behave differently, specialists may speak of “suspected VM”—a likely vestibular migraine that is not yet definitively confirmed.
What does that mean for you?
- Hearing problems or tinnitus point more toward Ménière’s; headache and light sensitivity point more toward vestibular migraine.
- A good diagnosis usually requires more than just one test.
- A thorough assessment saves time, wrong treatments, and uncertainty.
What Can You Do?
- Ask your doctor about vestibular tests (e.g., vHIT or caloric testing).
- Even if tests are normal: a second opinion at a specialized vertigo center can bring clarity.
🎯 Our IVRT®-certified dizziness and vestibular therapists support you with individualized balance training to regain confidence and well-being: IVRT therapist search