Vestibular disorders
Perilymph fistula
This information is intended as a general introduction to the topic. Since every person is affected differently by balance and dizziness problems, you should consult your doctor for individual advice.
For reasons of readability, the generic masculine form is used and the simultaneous use of the male, female, and diverse (m/f/d) forms is omitted. Unless otherwise specified, the personal designations used in this patient information refer to all genders.
What is a perilymph fistula?
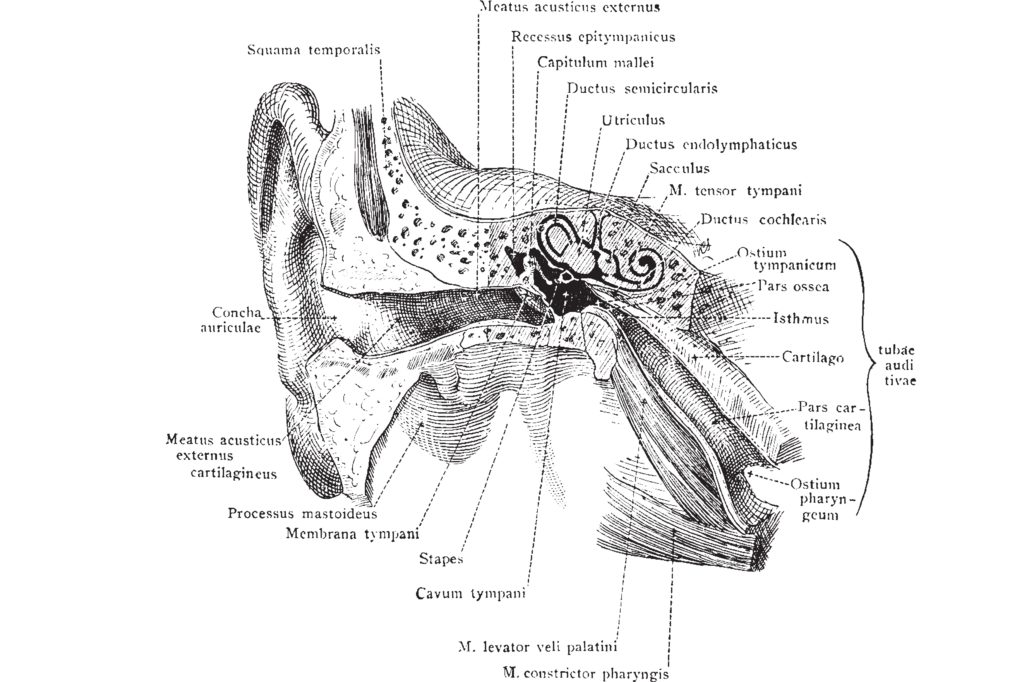
A fistula is an abnormal connection between two parts of the body. The perilymph is the fluid that fills the bony labyrinth in the inner ear.
A perilymph fistula is therefore an opening or tear in one or both membranes that separate the middle and inner ear. Perilymph can leak from the inner ear into the middle ear through this opening. It can occur in the oval or round window, in one of the semicircular canals (similar to semicircular canal dehiscence) or at another location.
A perilymphatic fistula can cause sudden or progressive hearing loss and dizziness.
Perilymphatic fistula is a controversial disease. Doctors and researchers disagree on how to define it, when it should be diagnosed and how it should be treated. There is no specific test to diagnose it, and the definition of perilymphatic fistula has changed over the years. In addition, the symptoms are similar to those of other inner ear disorders. But the diagnosis is becoming more widely recognized.
Perilymphatic fistula is rare. One group of researchers estimates that about 1.5 in 100,000 adults have perilymphatic fistula. It appears to be more common in children with sensorineural hearing loss that has no obvious cause (idiopathic).
Summary
- An abnormal opening or tear in one or both of the membranes separating the middle and inner ear.
- May cause sudden or progressive hearing loss and dizziness (vertigo).
- Rare and controversial disease, as not everyone agrees on the definition, diagnosis or treatment.
- It can be caused by an illness, a pressure injury or barotrauma, or for no apparent reason.
- Treatment may involve avoiding triggers, treating other conditions or surgery.
What causes a perilymph fistula?
Many different things can cause a perilymph fistula. Recently, the following four groups of causes have been identified:
- Illness (e.g. meningitis), trauma (e.g. minor traumatic brain injury) or surgery
- Pressure injury (barotrauma) caused by external forces (e.g. flying or diving)
- Pressure injury (barotrauma) caused by internal forces (such as straining, sneezing or coughing)
- No obvious cause (idiopathic)
A perilymph fistula can cause both vestibular and auditory disorders.
- Vertigo
- Balance disorders
- Nausea or vomiting
- Sudden or progressive sensorineural hearing loss that sometimes gets better or worse (fluctuating)
- Tinnitus
- Sensitivity to everyday noises (hyperacusis)
- Ffeeling of fullness or flowing water in the ear
Some people with perilymphatic fistula have problems perceiving complex environments such as crowds or traffic. They also have concentration and memory problems.
Some people with perilymphatic fistula find that their symptoms are triggered by loud noises. Symptoms may also be exacerbated by activities that cause pressure changes inside or outside the body, such as
- Cough
- Sneeze
- Blowing your nose
- Tighten
- Sport
- Flying
Diagnosis of a perilymph fistula
A perilymph fistula can be diagnosed by a neuro-otologist or ENT specialist who specializes in vertigo.
These specialized doctors will take a detailed medical history, perform a neurological examination, and carry out various tests to assess the function of your vestibular system.
You will probably undergo some of the following diagnostic tests:
- Hearing test and vestibular function tests
- Imaging such as magnetic resonance imaging (MRI) or computer tomography (CT); this can help to rule out diseases such as semicircular canal dehiscence (SCD syndrome)
Since many other diseases cause similar symptoms, the doctor must rule out diseases such as Meniere's disease or vestibular migraine before diagnosing perilymphatic fistula.
Treatment of perilymphatic fistula
Different doctors and researchers have different opinions on how best to treat a perilymph fistula. Some doctors believe that rapid treatment is necessary to achieve a good result. Others have found that patients can benefit from treatment even after years of disease development.
Therapy option
Avoid triggers
Some doctors prefer to wait a few months and see if the fistula heals on its own. During this time, you should avoid lifting heavy things, flying, playing wind instruments, scuba diving or anything else that could increase the pressure in your body. Your doctor may even suggest bed rest, although this is an outdated approach and many doctors no longer consider it necessary.
Therapy option
Treatment of other possible diseases
Your doctor may suggest trying some treatments for Meniere's disease or migraine, especially if the diagnosis of perilymphatic fistula is not clear.
Therapy option

Surgery
If your perilymphatic fistula is visible with imaging or if you have definitely had an injury or other event that may have caused the fistula, your doctor may suggest surgery to close the opening. Surgical treatment of perilymphatic fistula may involve the use of surgical glue, tissue grafting and/or laser surgery. It may be a simple procedure in your doctor's office or a more complicated surgery in a hospital. This depends in part on where the fistula is located.
Another surgical option for treating perilymphatic fistula is a pressure equalization tube (PE tube or tympanotomy tube). The surgeon makes a tiny hole in the eardrum on the same side as the fistula and then inserts a small, soft tube into the hole. This helps to equalize the pressure inside and outside the middle ear. This can help to protect the ear from external sources of pressure, e.g. when flying.
In extremely rare cases, if nothing else helps and the symptoms are unbearable, the doctor may suggest severing the vestibular nerve as a last resort.
A less invasive option is the injection of gentamicin, an antibiotic that destroys the cells in the vestibular part of the inner ear. In most cases, patients no longer have vertigo after this treatment. However, there is a risk of hearing loss with this treatment.
What happens next?
What you can expect in the future.
New tests are being developed for perilymphatic fistula. These tests look for a specific molecule (or biomarker) that is only found in the perilymph and is known as Cochlin's tomoprotein or CTP. To perform the test, a doctor takes a sample of fluid from the middle ear during a surgical procedure. A laboratory then analyzes the sample. If the test shows CTP in the fluid, it means that perilymph is leaking into the middle ear. However, only 1 in 5 cases of perilymph fistula is found with this test. The test is currently only available in Japan, but it may soon be approved in other countries.
In order to keep this patient information as short as possible, we have not included a detailed list of references. However, this can be requested at any time at info@ivrt.de.