Balance problems?
What exactly is balance?
Vestibular vertigo?
What is a vestibular disorder?
VESTIBULAR DISORDER
Treatment of dizziness & balance disorders
Some questions and their answers about vestibular disorders.
What is a vestibular disorder?
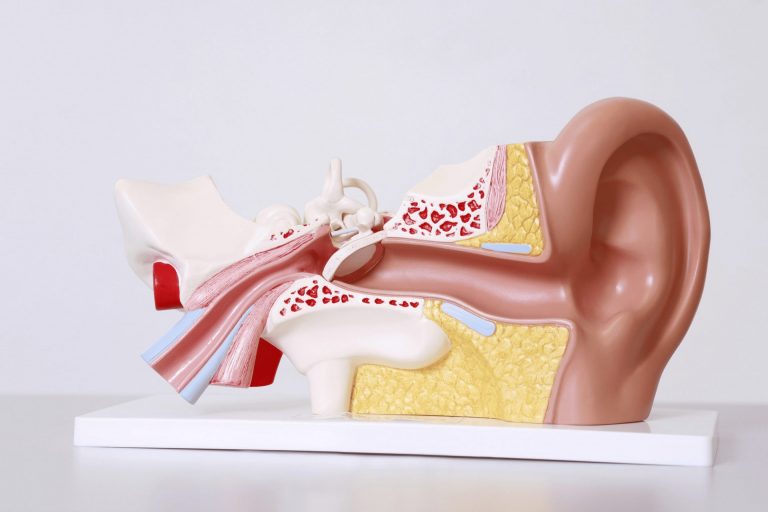
The vestibular system includes the parts of the inner ear and brain that process the information involved in balance control and eye movements. When a disease or injury damages these information-processing areas, a vestibular disorder can result. Vestibular disorders can also be caused or exacerbated by genetic or environmental factors. Development for unknown reasons is also possible.
Introductory exercises
Start with simple introductory exercises.
Questions
Please feel free to contact us if you have any questions.
Therapist search
Find a certified therapist directly on site.
What exactly is balance?
Balance is the ability to maintain the body's center of gravity over the body's center of support. A well-functioning balance system enables people to see clearly when moving, to determine orientation with respect to gravity, to determine the direction and speed of movement, and to maintain posture and stability under different conditions and activities through automatic postural adjustments.
Balance is achieved and maintained through a complex set of sensorimotor control systems. These systems include sensory input from the eyes (vision), proprioception (feeling/perception) and the vestibular system (movement, balance, spatial orientation). The integration of these sensory inputs and the motor outputs of the eyes and body muscles maintain balance. An injury, illness or the ageing process can affect one or more of these components.
The disease
Vestibular disorder
What are the symptoms of a vestibular disorder?
The vestibular system consists of the parts of the inner ear and brain that control balance and eye movements. When the system is damaged by disease, aging or injury, vestibular disorders can develop. These disorders are associated with one or more of these symptoms, among others:
- Dizziness and lightheadedness
- Impaired balance or spatial orientation
- Visual impairment
- Changes in hearing
- Cognitive and/or psychological changes
Not all symptoms will occur in every person with an inner ear disorder and other symptoms may also occur. An inner ear disorder can also be present without any obvious or severe symptoms. It is important to note that most of these individual symptoms can also be caused by other reasons.
The nature and severity of symptoms can vary considerably, be frightening and difficult to describe. People affected by certain symptoms of vestibular disorder may be perceived as inattentive, sluggish, overly anxious or attention-seeking. They may have problems with reading and simple arithmetic. Activities at work, school, daily routine tasks or getting up in the morning may be difficult for some.
Dizziness and lightheadedness
- A spinning or whirling sensation; the feeling that you or the world around you are spinning (vertigo)
- Lightheadedness, as well as a floating or swaying feeling
- The feeling of being heavy or being pulled in one direction
Balance and spatial orientation
- Impaired balance, stumbling, difficulty walking straight or turning a corner
- Clumsiness or coordination difficulties
- Difficulty maintaining a straight posture; tendency to look down to keep the ground in view
- The head is held at an angle
- The tendency to grab or hold something while standing; or to grab or hold the head while sitting
- Sensitivity to changes in the surface or footwear
- Muscle and joint pain (due to balance problems)
- Difficulty maintaining balance in crowds or in large, open spaces
Visual
- Difficulty fixing or tracking objects; objects or words on a page seem to jump, blur or appear twice
- Busy, visual environments such as traffic, crowds or stores are unpleasant
- Sensitivity to light, glare and moving or flickering lights; fluorescent light can be particularly unpleasant
- Sensitivity to certain computer or television screens
- Tendency to fixate close objects; fixating distant objects is unpleasant
- Increased night blindness; difficulty walking in the dark
- Weak depth perception
Auditory
- Hearing loss; distorted and fluctuating hearing
- Tinnitus (ringing, hissing, buzzing, hissing or other noises in the ear)
- Sensitivity to loud noises or noisy surroundings
- Sudden, loud noises can exacerbate symptoms such as dizziness or loss of balance
Cognitive
- Difficulty concentrating or reduced attention; easily distracted
- Forgetfulness and short-term memory impairment
- Confusion, disorientation; difficulty understanding instructions and directions
- Difficulty following the speaker during a conversation, meeting, etc., especially with loud background noise or movement in the background
- Mental and/or physical exhaustion that is disproportionate to activity
Psychological
- Loss of independence, self-confidence and self-esteem
- Anxiety, panic, social isolation
- Depression
Other symptoms
- Nausea or vomiting
- Feeling of having a "hangover" or being seasick
- Motion sickness
- Feeling of fullness in the ear
- Headache
- Indistinct language
- Sensitivity to pressure, temperature changes or wind currents
- Pain, pressure or other symptoms when changing diet (e.g. high sodium intake)
How are vestibular disorders diagnosed?
Doctors use the information from the personal medical history and the findings of the physical examination as a basis for ordering diagnostic tests to examine the function of the vestibular system and rule out alternative causes of the symptoms.
Specific tests for vestibular dysfunction
Good balance and clear vision rely on a close connection between the vestibular organs and the eyes. Head movements or other stimulation of the inner ear send signals to the eye muscles via the nervous system; this is called the "vestibulo-ocular reflex", or VOR for short. The VOR normally generates eye movements that ensure clear vision during head movements.
Electronystagmography (ENG)
The ENG is a battery of eye movement tests that look for signs of vestibular dysfunction or neurological problems by measuring nystagmus (a type of involuntary eye movement) and other eye movements. ENG tests are the most commonly performed tests for people with dizziness and/or balance disorders, although the test battery and some test methods can vary greatly from examiner to examiner.
During ENG, eye movements are recorded and analyzed using small electrodes placed on the skin around the eyes. The electrodes are self-adhesive, similar to a plaster bandage. Alternatively, eye movements can be recorded using video nystagmography (VNG). This is done using an infrared video camera mounted in special glasses that the patient puts on.
An ENG/VNG test evaluates eye movements as they follow a moving target object. They also observe eye movements at different head positions. During the caloric test (sometimes called bi-thermal caloric or mono-thermal caloric), warm water, cold water or air is circulated in the ear canal to test the nystagmus response stimulated by the temperature change.
Rotation tests
The rotation tests can also evaluate how well the eyes and inner ear work together. For every head movement in one direction, there is an eye movement in the opposite direction. Rotation tests, also using the ENG electrodes or VNG goggles, allow the examiner to record any eye movements as the head moves at different speeds. This provides additional information, beyond the ENG/VNG, about how well the balance organs and their connections to the eye muscles are functioning. Not all people need the rotation tests in the diagnostic phase.
Vestibular Evoked Myogenic Potentials (VEMP)
The VEMP examination is used to assess whether the sacculus and the lower vestibular nerve are intact and functioning normally. During the VEMP examination, the patient is fitted with headphones and small electrodes are attached to the skin of the neck muscles. When sounds are transmitted through the headphones, the electrodes record the muscle response to the vestibular stimuli.
Computer-aided dynamic posturography (CDP)
The CDP examines postural stability. While ENG/VNG and rotation tests assess visual-vestibular interaction, the CDP provides information on motor control and balance under different environmental conditions. This is very important because the ability to maintain balance relies not only on sensory information from the visual and vestibular systems, but also on sensory information received by the brain from the muscles and joints. These somatosensory signals provide information about, for example, the direction of head rotation or the ground conditions and inclination of the running surface. The CDP examines the relationship between these three sensory inputs. It also measures the balance and postural adaptation that a person shows in response to the variation in reliable information provided by the visual and somatosensory systems.
The test involves standing on a special measuring plate and usually a visual target. The measuring plate and/or the visual target move and while the person being tested tries to keep their balance, the pressure sensors under the measuring plate register the shift in body weight (body sway). A safety harness is worn during the test.
Hearing tests
Audiometry measures hearing function. Hearing tests are an important part of vestibular diagnostics due to the close relationship between the inner ear, hearing and the organ of balance. All the various hearing tests carried out by an audiologist are required. These tests are carried out in a soundproof booth. The patient puts on headphones with an integrated microphone so that the patient can remain in contact with the audiologist.
For certain people with a vestibular disorder, it is necessary to have their hearing checked at regular intervals. This is particularly the case if there are signs of hearing loss, a feeling of fullness in the ears or tinnitus (ringing in the ears or other noises).
Treatment of dizziness and balance disorders
The type of treatment prescribed for vestibular disorders depends on the symptoms, medical history, general health, examination by a qualified physician and diagnostic results. In addition to treating the underlying condition that may be contributing to the balance disorder, treatment may also include the following:
Vestibular rehabilitation therapy (VRT)
VRT uses specific head, body and eye exercises that are designed to retrain the brain. This allows the brain to recognize and process signals from the vestibular system and coordinate them with information from the eyes and proprioception. The choice and type of VRT exercises will vary from patient to patient.
(More information on vestibular rehabilitation therapy)
Canalith repositioning maneuvers (e.g. the Epley maneuver)
A special form of VRT is given for the treatment of benign paroxysmal positional vertigo (BPLS). This treatment is often called the Epley maneuver and consists of a series of specially designed head and trunk movements that cause the tiny, displaced otoliths to move to a location in the inner ear where they cannot cause symptoms.
(More information on the Epley maneuver)
Exercises for at home
Home exercises are often an essential part of the treatment. Physiotherapists or occupational therapists give patients appropriate VRT exercises to do at home, which must be performed at a set pace. The exercises should also be supplemented with progressive fitness training, which increases strength and reduces stress.
(More information on introductory exercises)
Change of diet
Many people with Meniere's disease, secondary endolymphatic hydrops and migraine-associated vertigo find that certain dietary modifications help them. Avoiding substances that the diet rejects, such as nicotine and certain medications, can also reduce symptoms.
Talk therapy - psychological counseling
Symptoms of vestibular disease are invisible and unpredictable. This does not mean that they are imaginary, but that they often contribute to a variety of psychological consequences. People with vestibular disease often need support and benefit from psychological counseling to better cope with lifestyle changes, depression, guilt and grief. This is because you can no longer meet your expectations or the expectations of others.
Medication
The use of medication for the treatment of vestibular disorders depends on whether the disorder of the vestibular system is in the initial or acute phase (lasts up to 5 days) or in the chronic phase (persistent).
Surgery
If medical treatment is not effective in controlling vertigo and other symptoms are caused by the vestibular system disorder, surgical intervention may be considered. The type of surgery depends on each individual's diagnosis and medical condition. Surgical interventions for peripheral vestibular disorders are either corrective or destructive. The aim of corrective surgery is to restore or stabilize the function of the inner ear. The aim of destructive surgery is to stop the production of sensory information or the transmission of this information from the inner ear to the brain.
Different vestibular diseases
Acoustic neuroma
An acoustic neuroma is a rare, benign tumor that develops on the vestibulocochlear nerve, which connects the inner ear to the brain. This tumor is most common in people between the ages of 30 and 60, but can occur at any age. It usually grows slowly, with unilateral hearing loss often being the first symptom. Other symptoms may include tinnitus, balance problems and dizziness. Treatment options include observation of the tumor, surgical removal or radiation. Vestibular rehabilitation after surgery can help to alleviate dizziness and balance problems. In rare cases, the tumor can become life-threatening if left untreated and becomes very large. It rarely returns after treatment.
(More information on acoustic neuroma)
Autoimmune inner ear disease
Autoimmune inner ear disease occurs when the immune system mistakenly attacks the inner ear. Most cases are primary and affect only the ear, while 30% are secondary and associated with a systemic autoimmune disease. Typically, there is fluctuating sensorineural hearing loss in one ear that worsens over days to months and eventually spreads to the other ear. Around half of those affected also suffer from balance problems and dizziness. Treatment usually involves corticosteroids or other immunosuppressive drugs. Vestibular rehabilitation can help with balance and dizziness problems. Hearing aids or later a cochlear implant may also be recommended.
(More information on autoimmune inner ear disease)
Bilateral vestibulopathy
Bilateral vestibulopathy is damage to the vestibular organs in both inner ears. The typical symptoms include balance disorders, an unsteady gait and "shaky" vision when moving the head. Hearing loss can occur, but does not necessarily have to be present. The balance problems often worsen when walking on uneven ground or in the dark. Certain medications should be avoided as they can exacerbate the damage, as well as unsafe situations to prevent falls. Vestibular rehabilitation can be helpful. While some people recover, others suffer from the condition for life.
(More information on bilateral vestibulopathy)
Benign paroxysmal positional vertigo
Benign paroxysmal positional vertigo (BPLS) is one of the most common causes of rotatory vertigo, occurring mainly in middle-aged and older people. It usually only affects one ear and increases the risk of falls. The condition is caused by tiny calcium carbonate crystals falling from the utriculus, a part of the inner ear, into one of the semicircular canals. These slipped crystals cause sudden, brief spinning vertigo triggered by certain head movements, such as lying down or turning over in bed. To stop the dizziness, the crystals must be brought back into the utriculus. This can be achieved by special release maneuvers performed by a doctor or vertigo and vestibular therapist. In most cases, only one treatment is necessary. Rarer forms of BPLS are more difficult to diagnose and treat. BPLS is unlikely if the spinning dizziness lasts longer than one minute.
(More information on benign paroxysmal positional vertigo)
Semicircular canal dehiscence
Dehiscence of the semicircular canal is a rare condition in which a hole develops in the bony covering of a semicircular canal in the inner ear, usually in the superior semicircular canal. It often occurs in older adults, but can occur at any age. This hole can occur during fetal development, from an injury or from thinning bones later in life. The condition causes both hearing and balance problems. Those affected often hear internal sounds such as their own voice, heartbeat or even eye movements. Avoiding triggers, tinnitus retraining therapy and a hearing aid can help to alleviate the symptoms. For severe symptoms, surgery to close the hole is recommended.
(More information on semicircular canal dehiscence)
CANVAS syndrome
CANVAS syndrome is a rare neurological syndrome that affects balance and occurs mainly in adults over the age of 50. It is a slowly progressive disorder that affects three areas: cerebellar ataxia (disruption of muscle control by the cerebellum), neuropathy (disruption of the nerves) and vestibular areflexia (impaired reflexes of the inner ear). If all three areas are affected, the balance problems can be particularly severe, although vertigo is not usually a symptom. Treatment focuses on controlling the symptoms and avoiding triggering factors. Vestibular rehabilitation can help the brain to compensate for the missing signals from the inner ear.
(More information on CANVAS syndrome)
Cholesteatoma
A cholesteatoma is a benign skin growth that forms in the wrong place in the middle ear, behind the eardrum. This rare and slow-growing disease can affect people of any age. A typical early symptom is a foul-smelling discharge from the ear. Other early signs include conductive hearing loss, pressure, pain or numbness in or around the affected ear, with hearing loss being the most common in children. If left untreated, a cholesteatoma can damage parts of the inner ear that are important for hearing and balance. Surgery is usually necessary and successful, although growth rarely returns. After the operation, the ear usually needs to be cleaned regularly by an ENT specialist for the rest of the patient's life.
(More information on the cholesteatoma)
Enlarged vestibular aqueduct
Enlarged vestibular aqueduct (EVA) is a congenital disorder in which the normally narrow canals that run from the inner ear into the skull are enlarged. This abnormality is thought to occur during fetal development due to a genetic problem. EVA can occur in isolation or in conjunction with other syndromes. Symptoms include sensorineural hearing loss, rotary vertigo and balance problems, with young people, especially infants through to people in their 20s, most commonly affected. Hearing protection is often recommended to prevent sudden hearing loss after a minor head injury or an extreme change in air pressure. There is no specific treatment to reduce or slow down hearing loss. A cochlear implant may be an option but carries certain risks.
(More information on the Enlarged vestibular aqueduct)
Isolated otolith dysfunction
Isolated otolith dysfunction is a collective term for disorders of the macular organ, which consists of the saccule and the utriculus. These otoliths in the inner ear transmit important information about head position and movement to the brain. Otolith dysfunction can occur in isolation or in conjunction with other problems of the vestibular system, particularly the semicircular canals. Symptoms include a misdirected sense of non-rotational movement, tilting movements and sudden attacks of falling. Two specific vestibular function tests are used to investigate the otoliths. Vestibular rehabilitation therapy aimed at activating the otoliths appears to be helpful. However, research is still ongoing to determine the best definition, diagnosis and treatment of this disorder.
(More information on isolated otolith dysfunction)
Labyrinth infarction
A labyrinthine infarction is a serious form of minor stroke that can be a warning sign of a major stroke. The artery that supplies the inner ear with oxygen-rich blood becomes narrowed or blocked. Symptoms include sudden dizziness, loss of balance and a sudden loss of hearing in one ear. As this is a medical emergency, the emergency number should be called immediately. It particularly affects people between their mid-50s and early 60s, but it can occur at any age, especially in people with other stroke risk factors. The diagnosis is usually made in an emergency room, and immediate treatment includes medication to prevent further damage and reduce the risk of a major stroke. It is important to attend all follow-up appointments as the risk of a major stroke is increased. Nevertheless, over 80% of patients with associated hearing loss have a positive outcome.
(More information on labyrinth infarction)
Labyrinthitis
Labyrinthitis is an inflammation of the inner ear, often caused by a viral infection. It leads to a sudden, severe attack of spinning vertigo, often accompanied by nausea, vomiting and hearing loss or hearing distortion. It is important to rule out other serious causes of sudden vertigo, such as a stroke. The acute phase usually lasts 2 to 3 days and usually subsides on its own, although supportive treatments can help. A return to normal everyday life, including work, is usually possible within 2 weeks. If dizziness and balance problems persist after several months, vestibular rehabilitation may be helpful. In some cases, permanent hearing loss may occur, in which case a hearing aid or possibly a cochlear implant may help.
(More information on labyrinthitis)
Mal de Débarquement Syndrome
Mal de Débarquement Syndrome (MdDS), which translates as "sickness of disembarking", is often triggered after long journeys in a boat, car, train or plane. It mainly affects middle-aged women and differs from the usual motion sickness. The main symptom is a constant feeling of motion, but this subsides with passive movement, such as in a moving car. The causes may be a problem with the vestibulo-ocular reflex (VOR), hormone level changes or a type of vestibular migraine. MdDS is usually a chronic condition that can last for weeks, months or even years. Treatment includes medication and vestibular rehabilitation, while experimental methods such as the VOR protocol and brain stimulation are also being considered.
(More information on Mal de Débarquement Syndrome)
Meniere's disease
Meniere's disease is a disease of the inner ear that can cause dizziness and hearing loss. The attacks usually last for several hours and usually only affect one ear. It is a chronic condition that most commonly occurs in people aged between 30 and 60 years. Common symptoms include hearing loss, tinnitus and a feeling of pressure in the affected ear. The intensity and type of symptoms vary from person to person, with attacks ranging from mild to severe. With lifestyle adjustments, the use of medication and vestibular rehabilitation, the symptoms and long-term impact on daily life can be well controlled in many cases.
(More information on Meniere's disease)
Vestibular neuritis
Vestibular neuritis is a sudden and severe attack of vertigo, often accompanied by nausea and vomiting, but without hearing loss. It is caused by a disorder of the vestibular nerve, which prevents signals that control balance from reaching the brain. The condition occurs as a single major event and is not recurrent. It most commonly affects people between the ages of 30 and 50, although it can occur at any age. During the acute phase, which usually lasts 2 to 3 days, supportive treatment is given. However, balance problems and gait instability can persist for several weeks or months. Vestibular rehabilitation can support the recovery process. Recurrence is rare and most sufferers make a full recovery.
(More information on neuritis vestibularis)
Otosclerosis
Otosclerosis is a complex disorder in which there is abnormal bone growth in the middle ear. This growth causes the tiny bones that conduct sound to fuse with the surrounding bones, usually affecting both ears. Otosclerosis is one of the most common causes of conductive hearing loss in young adults, and the speed and extent of hearing loss is unpredictable. If the bone growth extends into the inner ear, it can also cause dizziness and balance problems. Hearing aids are usually the first choice for treatment, with 80% of patients improving their hearing after minimally invasive surgery. A healthy lifestyle can help to better manage the challenges that come with unexpected hearing loss.
(More information on otosclerosis)
Perilymph fistula
A perilymphatic fistula is an abnormal opening or tear in one or both of the membranes separating the middle and inner ear. This disorder can lead to sudden or progressive hearing loss and vertigo, especially spinning vertigo. Although rare, perilymphatic fistula is a controversial condition, with experts disagreeing on its definition, diagnosis or treatment. The causes can be varied, including disease, external or internal pressure injuries, or it can occur for no apparent reason. Treatment often involves avoiding triggers, treating underlying conditions or, in some cases, surgery.
(More information on perilymphatic fistula)
Persistent postural-perceptual dizziness
Persistent postural-perceptual dizziness (PPPD) is a common cause of long-lasting dizziness that can last three months or longer. In some people, PPPD develops after a triggering event, such as another balance disorder. Instead of fully recovering, the brain remains in a state of high alert and overreacts to stimuli. Often, the anxiety begins to be exacerbated by certain triggers, which can significantly interfere with daily life. This leads to a vicious circle: the more the anxiety increases, the more severe the symptoms become. It is important to note that the symptoms are real and do not represent a mental illness. Treatment for PPPD usually involves "retraining" the brain through vestibular rehabilitation, medication and counseling. Although there is no quick fix, with time, understanding and the right treatment, a cure is possible.
(More information on persistent postural-perceptual dizziness)
Presbyvestibulopathy
Presbyvestibulopathy, also known as age-related dizziness and gait unsteadiness, is one of the most common problems in older people. It has many causes that often overlap, including age-related deterioration of balance and other body systems. This disorder is often exacerbated by one or more other conditions that can affect balance function. Taking four or more medications increases the risk, as does an unsteady gait, fear of falling, loss of muscle mass, vision problems, dehydration, blood pressure abnormalities, thought disorders, bladder or bowel disease, foot problems, alcohol use, degenerative brain disease and heart disease. It is important to consult a doctor if you have symptoms, as these could be a sign of serious health problems. Presbyvestibulopathy can be dangerous if it causes a fall and can severely limit quality of life. Fortunately, there are many ways to treat and alleviate these symptoms.
(More information on presbyvestibulopathy)
Motion sickness and cyber sickness
Motion sickness is caused by being in a moving vehicle, while cyber sickness is triggered by viewing moving content on digital devices. In both cases, nausea or discomfort occurs, which usually subsides within a few hours after the motion or digital session ends. This discomfort is caused by a sensory mismatch or contradiction between the signals that the vestibular system sends to the brain. When such situations are unavoidable, various strategies can help reduce the symptoms. Vestibular rehabilitation can train the brain to adapt to these triggers. In addition, certain medications can be taken prophylactically to prevent or alleviate motion sickness.
(More information on motion sickness and cyber sickness)
Dizziness after a traumatic brain injury
After a mild traumatic brain injury (TBI), the vestibular system, i.e. the balance system, can be damaged. A TBI can affect both the balance-relevant structures of the inner ear and the brain, or both. The symptoms that occur depend on which parts of the vestibular system are affected. The assessment and treatment of dizziness after a TBI must be individualized. Most sufferers make a full recovery, but a minority suffer from persistent symptoms known as post-commotion syndrome.
(More information on dizziness and balance disorders after a mild traumatic brain injury)
Vestibular migraine
Vestibular migraine is characterized by repeated attacks of vertigo, usually without concurrent headaches. It is the second most common cause of dizziness and affects around 1 in 100 people. The vestibular symptoms include spinning vertigo, unsteadiness of gait or dizziness triggered by head movements and other factors. The severity and combination of symptoms can vary from seizure to seizure. These seizures usually last from several hours to days and can have a significant impact on daily life. Because the symptoms often resemble other conditions, vestibular migraine is often unrecognized or misdiagnosed. An accurate diagnosis can usually only be made by a specialist who is familiar with vestibular migraine. Treatment involves avoiding triggers, making lifestyle changes and taking medication to stop or mitigate attacks. Vestibular rehabilitation can be helpful, but should only be considered once attacks are well controlled. Continued treatment can significantly improve quality of life and both treat and prevent seizures.
(More information on vestibular migraine)
Vestibular paroxysmia
Vestibular paroxysmia is a disorder characterized by short, recurring bouts of vertigo. It is most common in people in their 40s and 50s, but can occur at any age. It is caused by damage or pressure on the vestibulocochlear nerve, which carries signals from the inner ear to the brain. The seizures usually occur without warning and last less than a minute. This condition is uncommon and usually chronic. It can often be treated with anticonvulsant medication, but in some cases surgery is considered.
(More information on vestibular paroxysmia)
Vestibulotoxicity
Vestibulotoxicity refers to temporary or permanent damage to the vestibular organ caused by certain drugs and chemicals, but fortunately it is rare. Unborn babies, very young children, the hearing impaired and the elderly are particularly at risk. This damage can be caused by aminoglycoside antibiotics, platinum-based chemotherapy drugs, mefloquine, solvents, organophosphates and heavy metals. In the treatment of life-threatening diseases, such as malignant tumors and severe infections, exposure may be unavoidable, while in other cases non-toxic alternatives may prevent harm. Some of these substances damage both the vestibular and auditory systems, while others affect only one of the two. Once vestibular or hearing functions are lost, they cannot be restored, so early diagnosis is crucial to prevent permanent damage. Vestibular rehabilitation is the most effective treatment for balance disorders, and hearing aids or a cochlear implant can help with hearing loss.
(More information on vestibulotoxicity)
Visually induced dizziness
Visually induced vertigo is a collective term for symptoms such as chronic dizziness or gait unsteadiness caused by vestibular disorders, which often occur when looking at complex patterns or movements. These symptoms can be distressing and disabling. Treatment varies depending on the cause, but often includes vestibular rehabilitation and visual habituation exercises. Patience and time are crucial, as ignoring the symptoms can make them worse. It is important to remain active as inactivity does not promote recovery.
Vestibular diseases
In this overview, we present various vestibular disorders that affect the vestibular organ and can cause a range of symptoms such as dizziness, balance disorders and nausea. Our compilation includes both common and less common disorders that are often challenging to diagnose and treat. The aim of this overview is to promote a deeper understanding of the complexity of these disorders and to provide valuable information for professionals and patients. Both the pathophysiological basis and current therapeutic approaches are highlighted.
























Thank you
Disclaimer
Dear colleagues, although the Imprint emphasizes that the texts on this website are protected by copyright, it unfortunately happens that my texts are copied without permission. I would therefore like to remind you that people who violate copyright law will be warned. This usually results in warning fees in the three-digit range and legal fees. The resulting economic damage can also be claimed.