Vestibular disorders
Autoimmune inner ear disease
This information is intended as a general introduction to the topic. Since every person is affected differently by balance and dizziness problems, you should consult your doctor for individual advice.
For reasons of readability, the generic masculine form is used and the simultaneous use of the male, female, and diverse (m/f/d) forms is omitted. Unless otherwise specified, the personal designations used in this patient information refer to all genders.
What is an autoimmune disease of the inner ear?
Normally, the immune system protects us from pathogens such as bacteria and viruses. But in an autoimmune disease, the immune system inadvertently attacks the body's own tissue. Autoimmune inner ear disease occurs when the immune system attacks tissue in the inner ear. This often leads to sensorineural hearing loss. Around 1 in 2 people affected also experience balance problems.
In most cases, only the ears are affected. This is known as primary autoimmune inner ear disease. However, it sometimes occurs as part of another autoimmune disease that also affects the rest of the body. This is called secondary autoimmune inner ear disease.
Summary
- Autoimmune inner ear disease occurs when the immune system inadvertently attacks the inner ear.
- Most cases are primary and affect only the ear.
- 30% of cases are secondary and are associated with an autoimmune disease that affects the whole body.
- Frequently, there is a fluctuating (fluctuating) sensorineural hearing loss in one ear, which usually worsens over several days to months.
- Half of those affected have problems with balance and dizziness.
- Treatment is usually with corticosteroids or other immunosuppressive drugs.
- Vestibular rehabilitation can help with balance and dizziness problems.
- Hearing aids and possibly later a cochlear implant may be recommended.
What causes autoimmune inner ear disease?
The immune system consists of many different cells and organs that protect our body from germs, parasites and other harmful influences. Part of how the immune system works is to distinguish between "endogenous" structures and "exogenous" structures. Specialized blood cells, known as B cells, produce proteins called antibodies. These attach themselves to "foreign" structures and alert other parts of the immune system to attack them.
However, sometimes the immune system makes a mistake: it forms antibodies (so-called autoantibodies or "self-antibodies") that attach themselves to the body's own proteins. Normally, the immune system would ignore these self-proteins. But if the autoantibodies incorrectly classify an organ or tissue as "foreign", other parts of the immune system see it as a threat and attack it. This leads to an autoimmune disease. There are many different autoimmune diseases, and many different organs and tissues can be affected.
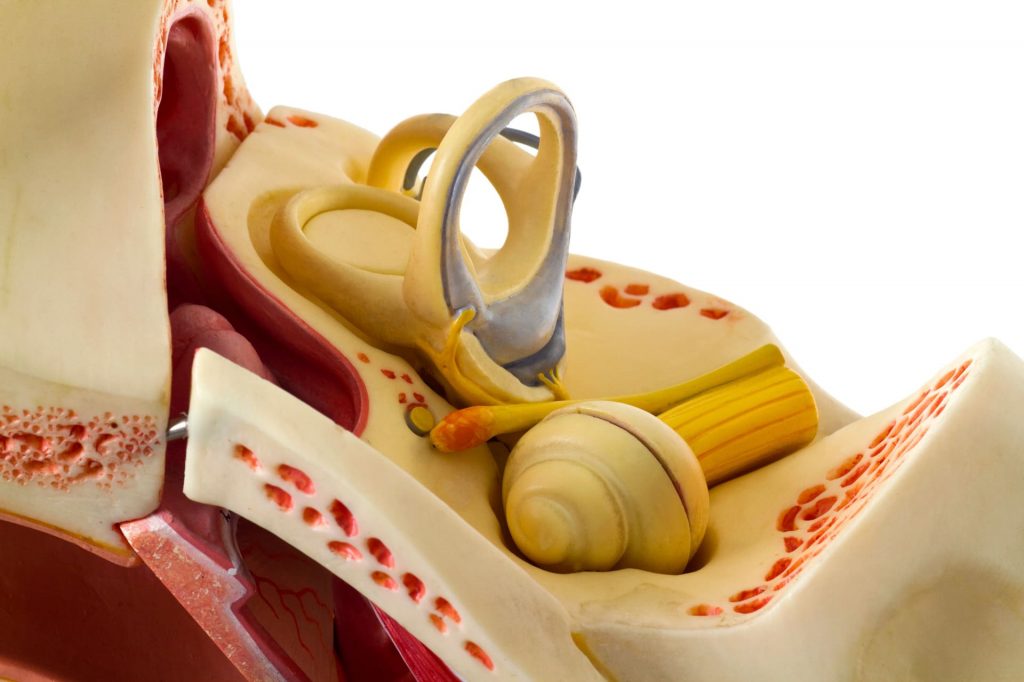
Science is still investigating the causes of autoimmune inner ear diseases. It is not exactly clear why and how the immune system recognizes the inner ear as foreign and attacks it. However, the attack appears to cause inflammation and damage to the cochlea (cochlea) and the vestibular organ (the organ of balance).
The autoimmune inner ear disease affects around 15 in 100,000 people.
About 3 out of 10 cases are secondary. This means that they are caused by an autoimmune disease that affects the whole body (systemic autoimmune disease). Many different systemic autoimmune diseases can cause secondary autoimmune inner ear disease, including:
- Ankylosing spondylitis (Bechterew's disease)
- Behçet's disease
- Cogan syndrome
- Recurrent polychondritis
- Rheumatoid arthritis
- Scleroderma (systemic sclerosis)
- Sjögren's syndrome
- Systemic lupus erythematosus
- Ulcerative colitis
- Vitiligo
- Vogt-Koyanagi-Harada syndrome
- Wegener's granulomatosis (Wegener's disease)
Autoimmune inner ear disease causes sensorineural hearing loss, which usually occurs suddenly and worsens over 3 days to 3 months. The hearing loss may initially affect only one ear. It often fluctuates, gets worse and spreads to the other ear over time. Some people also have tinnitus or a feeling of fullness in the ears.
About half of the patients also have vestibular disorders, such as:
- Vertigo; in some cases this only occurs when the head is in a certain position (positional vertigo) or it can come and go (episodic vertigo)
- Gait instability or balance problems
- Problems with muscle control and coordination (ataxia)
Diagnosis of autoimmune inner ear disease
The autoimmune inner ear disorders can be diagnosed by a neuro-otologist or otolaryngologist who specializes in vertigo. These specialized doctors will take a thorough medical history, perform a neurological examination and various tests to assess the function of your vestibular system.
You will probably undergo some of the following diagnostic tests:
- Hearing tests
- Vestibular functional examination
- Blood tests
- Imaging (MRI scans)
Some of these tests are performed to rule out other health problems. Other conditions can cause the same symptoms as autoimmune inner ear disease. Therefore, all possibilities must be considered before a diagnosis is made. The doctor will probably look for a pattern of test results and your medical history (how your condition has developed and changed over time).
Immune suppressing drugs such as steroids are often prescribed afterwards. If your symptoms improve under treatment, this can help to establish a diagnosis of autoimmune inner ear disease. But these medications don't always help.
There is still debate about the definition of autoimmune inner ear disease and how best to diagnose it. One group has proposed the following major and minor criteria. The group suggests that the diagnosis can be made if the patient fulfills at least three of the major criteria OR two major criteria and at least two minor criteria. However, these criteria are not used by all physicians.
Proposed main criteria:
- bilateral (both sides) hearing loss
- systemic autoimmune disease
- a high level of a type of autoantibody called antinuclear antibodies
- lower levels of certain white blood cells, the so-called T-naive lymphocytes
- More than 80 % restoration of hearing on treatment
Proposed secondary criteria:
- Unilateral (one-sided) hearing loss
- young or middle-aged patient
- female patients
- less than 80 % restoration of hearing with the treatment
Treatment of autoimmune inner ear diseases
The treatment is complicated. You may need to see several specialists, including an ENT specialist or a rheumatologist. Treatment usually consists of medication and hearing tests to see if the treatment is working. If the medication doesn't help and your hearing loss becomes too severe, your ENT specialist may recommend a hearing aid and later a cochlear implant.
Therapy option
Corticosteroids
The doctor will probably first prescribe you a high-dose steroid (such as prednisone) for at least four weeks. Steroids suppress the immune system and reduce inflammation. This treatment can reverse hearing loss in some people with autoimmune inner ear disease, but not all.
If steroid treatment helps, the medication should be taken for a longer period of time before slowly reducing the dose over days or weeks. People with a systemic autoimmune disease will probably need to take steroids for at least a year. However, steroids can have side effects if taken in high doses over a long period of time. Therefore, your doctor will need to find a balance between treating the autoimmune inner ear disease and managing the side effects.
Steroids can initially help about 7 in 10 people with autoimmune inner ear disease. However, over time, steroids help fewer and fewer people. Some studies have shown that only about 14% of those affected benefit from steroid treatment in the long term.
Therapy option
Immunosuppressive drugs
If steroids don't work, your doctor may suggest a drug that suppresses the immune system, such as cyclophosphamide. Cyclophosphamide can help treat autoimmune inner ear disease, but it can have serious side effects, such as infections, bladder cancer or infertility.
If steroids don't work, your doctor may suggest a drug that suppresses the immune system, such as cyclophosphamide. Cyclophosphamide can help treat autoimmune inner ear disease, but it can have serious side effects, such as infections, bladder cancer or infertility.
Therapy option

Hearing tests
During treatment, you will need to have regular hearing tests (audiometry) to determine whether your hearing is improving or deteriorating. You will need to repeat these tests often until your hearing has stabilized.
Therapy option
Vestibular rehabilitation & Dealing with dizziness and balance symptoms
If you have dizziness and/or balance problems, tests to check vestibular function will be carried out from time to time. Your treatment team may also recommend maneuvers for positional vertigo or vestibular rehabilitation if you need it.
What happens next?
What you can expect in the future.
Some researchers are working on new treatments, including gene therapy and the direct injection of anti-inflammatory drugs (such as steroids) into the inner ear. However, it will probably be several years before these treatments are available. They need to be carefully studied to ensure that they are effective and safe.
In order to keep this patient information as short as possible, we have not included a detailed list of references. However, this can be requested at any time at info@ivrt.de.