Vestibular disorders
Acoustic neuroma
This information is intended as a general introduction to the topic. Since every person is affected differently by balance and dizziness problems, you should consult your doctor for individual advice.
For reasons of readability, the generic masculine form is used and the simultaneous use of the male, female, and diverse (m/f/d) forms is omitted. Unless otherwise specified, the personal designations used in this patient information refer to all genders.
What is an acoustic neuroma?
An acoustic neuroma is a benign (non-cancerous) tumor of the vestibulocochlear nerve (also called the eighth cranial nerve). It usually grows slowly. The vestibulocochlear nerve transmits balance and hearing information from the inner ear to the brain. This means that as the tumor grows, it can cause hearing loss and tinnitus on the affected side, as well as dizziness and balance problems.
An acoustic neuroma is also called a vestibular schwannoma.
An acoustic neuroma affects about 1 in 100,000 people each year. It occurs most often in people between the ages of 30 and 60, but it can develop at any age.
If an acoustic neuroma becomes very large, it can affect the brainstem and the cerebellum. These parts of the brain help control basic body functions such as breathing, heartbeat, sleep, eating, and movement. This means that, in very rare cases, an acoustic neuroma can become life-threatening if it is not treated.
Summary
- A rare benign (non-cancerous) tumor on the vestibulocochlear nerve, which runs from the inner ear to the brain.
- It occurs most frequently in people between the ages of 30 and 60, but it can develop at any age.
- It usually grows slowly.
- The most common initial symptom is hearing loss in one ear.
- Other symptoms include tinnitus (ringing in the ear), balance disorders, and dizziness (usually vertigo attacks at the beginning, later unsteadiness and oscillopsia).
- Treatment options include “wait and see” (observation), surgical removal, or radiation therapy of the tumor.
- Vestibular rehabilitation shortly after surgery can help with dizziness and balance problems.
- In rare cases, it can become life-threatening if the tumor grows very large and is not treated.
- It rarely returns after treatment.
What causes an acoustic neuroma?
An acoustic neuroma develops when the cells that wrap around the vestibulocochlear nerve begin to grow uncontrollably. These cells are called Schwann cells. They produce a substance called myelin, which works like insulation around an electrical wire and helps the nerves transmit information through the body.
Scientists believe that Schwann cells begin to grow uncontrollably because of a change in the genetic code (a mutation) on chromosome 22. The affected gene controls the growth of Schwann cells.
In most cases, an acoustic neuroma occurs sporadically, and the tumor is present in only one ear.
In some cases, however, an acoustic neuroma occurs as part of a syndrome called neurofibromatosis type 2 (NF2). When an acoustic neuroma develops as part of NF2, tumors usually appear in both ears, not just one. NF2 causes tumors to grow in the brain and on many different nerves, not only on the vestibulocochlear nerve. In people with NF2, the first symptoms usually appear during the teenage years or as young adults. About half of the people with NF2 inherit the condition from one of their parents. The other half seem to develop it spontaneously, meaning that no one else in the family has the condition.
An acoustic neuroma usually presents with the following symptoms:
- Hearing loss in one ear or asymmetrical hearing loss (more in one ear than the other), which can occur either suddenly or progressively
- Tinnitus
- Coordination disorders
- Dizziness (usually vertigo attacks at the beginning, later unsteadiness and oscillopsia).
- Balance disorders
Many of these symptoms can also be caused by other conditions, so it is not always easy to diagnose an acoustic neuroma, especially in the early stages. However, asymmetric signs and symptoms (more pronounced on one side than the other) are often caused by an acoustic neuroma, which is why a healthcare professional will always want to rule out an acoustic neuroma during diagnosis.
As the tumor grows, it can press on other nearby nerves, such as the facial nerve and the trigeminal nerve. This can cause various problems, such as:
- Numbness, tingling in the face
- Weakness or paralysis of the facial muscles
- Double vision
- Difficulty swallowing or speaking
Diagnosis of an acoustic neuroma
An acoustic neuroma is usually diagnosed by a specialist such as a neurologist or an ear, nose and throat specialist.
Your doctor will ask you about your symptoms and medical history. You will also undergo a thorough physical and neurological examination, including an examination of the ears.
You will likely undergo the following diagnostic tests:
- Hearing and balance tests (audiogram, vestibular function tests and brainstem responses)
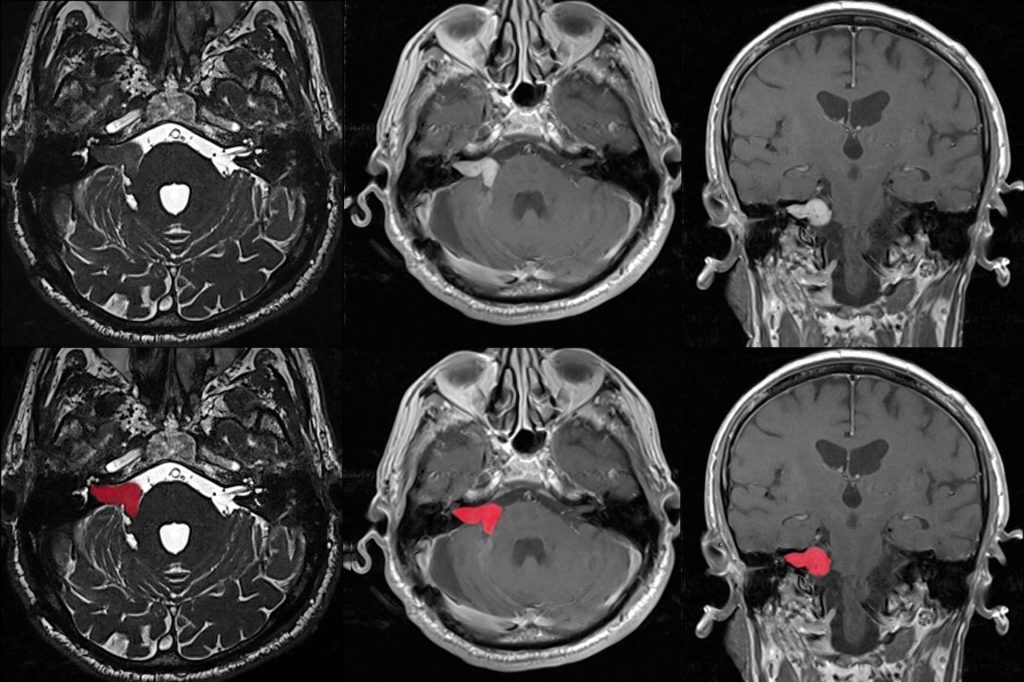
- Imaging (MRI scan)
When asymmetric hearing and balance symptoms occur, an imaging test is always ordered to rule out an acoustic neuroma. An MRI scan with contrast dye (gadolinium) is the gold standard for diagnosing an acoustic neuroma. This allows very small tumors to be detected that might otherwise go unnoticed without a contrast-enhanced MRI.
Treatment of acoustic neuroma
If the acoustic neuroma is small and causes only mild symptoms, your doctor may suggest monitoring it for a period of time to see if it grows or causes further symptoms (“wait and see”). This means you will have regular follow-up appointments and MRI scans. If anything changes, your doctor may decide that treatment is necessary.
Therapy option
Observation
If the acoustic neuroma is small and causes only mild symptoms, your doctor may suggest monitoring it for a period of time to see if it grows or causes further symptoms (“wait and see”). This means you will have regular follow-up appointments and MRI scans. If anything changes, your doctor may decide that treatment is necessary.
Therapy option
Surgery
If the acoustic neuroma is small, it may be possible to remove it by surgery. If the operation goes well, it can preserve hearing and improve other symptoms.
If the acoustic neuroma is larger, it may have already damaged the vestibulocochlear nerve and other nearby nerves. This means that surgery may be more difficult or may not relieve the symptoms.
The operation should be performed by a neurosurgeon who specializes in the removal of acoustic neuromas. There are several different surgical options. Which procedure is used depends on various factors, e.g:
- how large the acoustic neuroma is
- what symptoms it causes
- how much it affects your hearing
- how experienced the surgeon is with the respective procedure
Surgery for an acoustic neuroma can sometimes worsen the symptoms, as the vestibulocochlear nerve and other nearby nerves may be damaged. Compared to other treatment options, surgery carries a higher risk of permanent hearing and balance function loss.
Therapy option

Radiation treatment
During radiation treatment, high doses of radiation are directed into a small area of the body. The aim is to kill the tumor cells without damaging the healthy parts of the body nearby. Radiation treatment is often a good option for small, non-malignant tumors such as acoustic neuromas. Compared to surgery, it may be a better option for preserving your hearing.
Radiation treatment may be recommended if:
- you would prefer not to have surgery or surgery is not a good option for you
- the acoustic neuroma affects your only hearing ear or you have acoustic neuromas that affect both ears
There are two options for radiation treatment:
- stereotactic radiosurgery, i.e. a single, targeted dose of radiation
- radiotherapy in which several low doses of radiation are administered over several days
Therapy option
Vestibular rehabilitation
Surgery for an acoustic neuroma can damage your vestibular nerve. This can lead to balance problems, vertigo and oscillopsia. Vestibular rehabilitation shortly after surgery can help with these problems.
Vestibular rehabilitation is an exercise therapy. Its goal is to help your brain compensate for the loss of balance function on one side. Vestibular rehabilitation will help your brain to relearn balance control and respond to signals from the visual and vestibular systems. For many patients, this rebalancing happens naturally, so they do not need vestibular rehabilitation. However, other patients may continue to have symptoms and therefore benefit from vestibular rehabilitation exercises. One study found that patients who underwent an individualized vestibular rehabilitation program after acoustic neuroma surgery performed better on balance tests than patients who received only general instructions. A certified IVRT® Dizziness and Vestibular Therapist can help you create a program that is right for you.
It is very important that you start the exercises gradually and increase them slowly and steadily. If you try to do too much too quickly, your dizziness can get worse.
Therapy option

Facial muscle training
In rare cases, when an acoustic neuroma is removed, the facial nerve that leads from the affected side to the brain is damaged. This results in paralysis or drooping on one side of your face. Facial muscle training, sometimes called neuromuscular re-education, utilizes your brain's ability to change and adapt based on experience (neuroplasticity). The active and persistent cooperation of the patient is necessary to train the brain while the nerve regenerates. The goals of facial muscle training are a more symmetrical face, regaining control of the muscles used for facial expression and a greater range of movement in the face. A physiotherapist or speech therapist who specializes in facial muscle therapy can help you develop a suitable program for you.
It is important to practise the exercises regularly at home to improve the symptoms.
What happens next?
What you can expect in the future.
If you have had surgery or radiation, you will need to have regular follow-up visits, including MRI scans and hearing tests, to make sure nothing has changed. It is very rare for an acoustic neuroma to recur after treatment.
Many people still have hearing loss, tinnitus, vertigo, oscillopsia or other symptoms after treatment:
- One study found that 8 years after treatment for acoustic neuroma, 3 out of 4 patients were still deaf in the affected ear. People who already had some hearing loss before treatment were more likely to lose their hearing completely.
- Another study found that eight years after treatment, around 1 in 2 patients still had symptoms of dizziness. People who already had a major tumor or suffered from dizziness, headaches or migraines before the treatment had a higher risk of still suffering from dizziness later on. Vestibular rehabilitation can help to reduce dizziness.
In order to keep this patient information as short as possible, we have not included a detailed list of references. However, this can be requested at any time at info@ivrt.de.